- BriaCell doubles Progression-Free-Survival (PFS) and Clinical Benefit Rate vs historical results in the literature
- Bria-IMT™ PFS compares favorably to PFS of most recent treatment in 48% of Antibody-Drug Conjugate (ADC) resistant patients
- Therapy well-tolerated with no Bria-IMT™ related discontinuations
- Clinical data highlight significant potential of Bria-IMT™ in advanced metastatic breast cancer
- Superiority of selected Phase 3 regimen and formulation confirmed
- Oral presentation by Mayo Clinic Professor and Principal Investigator, Saranya Chumsri, MD, on Monday June 3; 11:30 AM-1:00 PM CDT
PHILADELPHIA and VANCOUVER, British Columbia, June 03, 2024 (GLOBE NEWSWIRE) — BriaCell Therapeutics Corp. (Nasdaq: BCTX, BCTXW) (TSX: BCT) (“BriaCell” or the “Company”), a clinical-stage biotechnology company that develops novel immunotherapies to transform cancer care, announces positive clinical efficacy data updates of its ongoing randomized Phase 2 study evaluating lead clinical candidate Bria-IMT™ in patients with advanced metastatic breast cancer. Two poster sessions, one abstract, and one oral presentation session (by Principal Investigator and Professor of Oncology, Mayo Clinic, Saranya Chumsri, MD), will be presented at the 2024 American Society of Clinical Oncology (ASCO) Annual Meeting taking place today June 3, 2024 at McCormick Place, Chicago, IL.
“We are very impressed with both clinical efficacy and safety data in these heavily pretreated patients. Given the limited effective treatment options in this group of patients, and the fact that most treatments are associated with significant toxicities, physicians and patients often opt to decline further ineffective and toxic drugs in lieu of palliative care,” Saranya Chumsri, MD, Principal Investigator and Professor of Oncology, Mayo Clinic. “Antibody-drug conjugates (ADCs) and immune checkpoint Inhibitors (CPIs) have emerged as the latest therapies to treat these patients. However, a large percentage of late-stage patients do not respond, and all patients inevitably develop resistance to them, making a safe and effective treatment an urgent medical need. BriaCell’s novel immunotherapy offers a well-tolerated treatment option for these patients beyond the currently approved drugs.”
“While immunotherapy has emerged as an active treatment option for multiple cancer types, its use in breast cancer is rather restricted to a minority of patients. Discovering new strategies, in order to enhance the responsiveness of various subtypes of breast cancer to immunotherapy, presents as a therapeutic opportunity. Through its unique mechanism of action, Bria-IMT™ regimen selectively activates adaptive cancer-fighting CD4+ and CD8+ T cells and innate responses (dendritic and NK cells) to activate patients’ immune systems without producing serious side effects,” stated Carmen Calfa, M.D., Clinical Research Lead for the breast site disease group at the University of Miami Miller School of Medicine, Co-Director of the Cancer Survivorship Program at Sylvester Comprehensive Cancer Center, and Principal Clinical Investigator of the Phase 2 Bria-IMT™ study.
“Our ASCO presentations highlight how Bria-IMT™’s activities – through diverse mechanisms including adaptive and innate responses – synergize with multiple mechanisms of action of checkpoint inhibitors,” stated Dr. Williams, BriaCell’s President and CEO. “We believe Bria-IMT™ has the potential to become a breakthrough novel treatment option for patients in advanced metastatic breast cancer.”
The details of the presentations are summarized below.
Oral Presentation Summary
Abstract Number for Publication: 1022
Title: Outcomes of advanced/metastatic breast cancer (aMBC) treated with Bria-IMT™, an allogeneic whole cell immunotherapy.
Session Type and Title: Rapid Oral Abstract – Breast Cancer—Metastatic
Session Date and Time: 6/3/2024; 11:30 AM-1:00 PM CDT
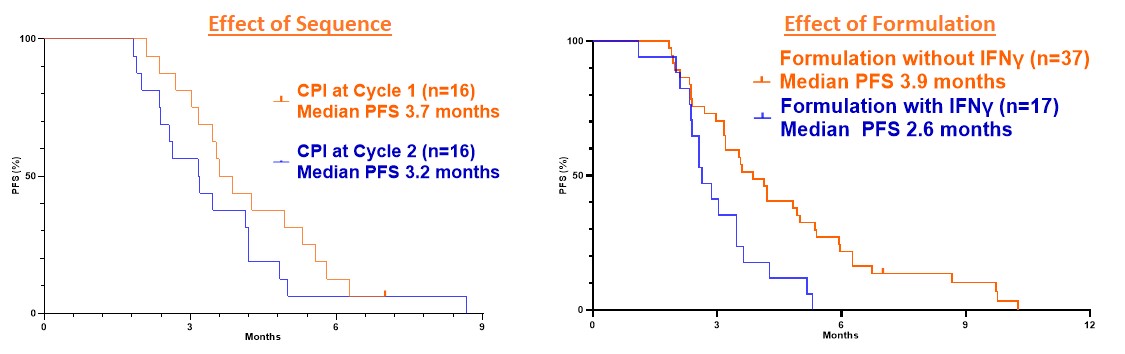
This presentation details the results of BriaCell’s randomized Phase 2 study of Bria-IMT™ in combination with retifanlimab, an immune checkpoint inhibitor (CPI). The goal of randomization was to compare whether administration of the CPI early, in the first cycle of therapy, or later, late in the second cycle of therapy, offered any advantage. Two different formulations of Bria-IMT™ were also evaluated; one treated with interferon gamma and one untreated.
The patients entering the study were very heavily pretreated and had failed multiple prior therapies as shown in the Table 1 below.
| Table 1. Prior Therapies in the Bria-IMT™ Phase 2 Study |
|
| Previous Therapies | Number of Patients (%) |
| Antibody-Drug Conjugates (ADC) | 23 (44%) |
| Immune Checkpoint Inhibitor (CPI) | 11 (20%) |
| Cyclin-Dependent Kinase (CDK) 4/6 Inhibitors | 34 (63%) |
A total of 54 patients were included in the Phase 1/2 study. Nearly half of these had been treated previously with an antibody drug conjugate and had progressed in their disease following this treatment. Another 20% had failed a prior immune checkpoint inhibitor. Nearly 2/3 of the patients had failed therapy with a CDK 4/6 inhibitor. On average they had failed six prior therapy attempts.
In the Phase 2 portion of the study, there were 32 patients with 16 treated with CPI early and 16 treated with CPI late. There was no statistically significant difference in progression-free survival (PFS) two groups. However, a slight advantage in the CPI early group has led this to be the selected regimen for the Phase 3 study. In the entire Phase 1/2 experience, with 54 patients, the formulation not incubated with interferon gamma showed a statistically significant improvement in PFS. Therefore, this formulation was selected for the Phase 3 study. The data are shown in Figure 1.
Figure 1. Effect of treatment sequence and formulation on PFS
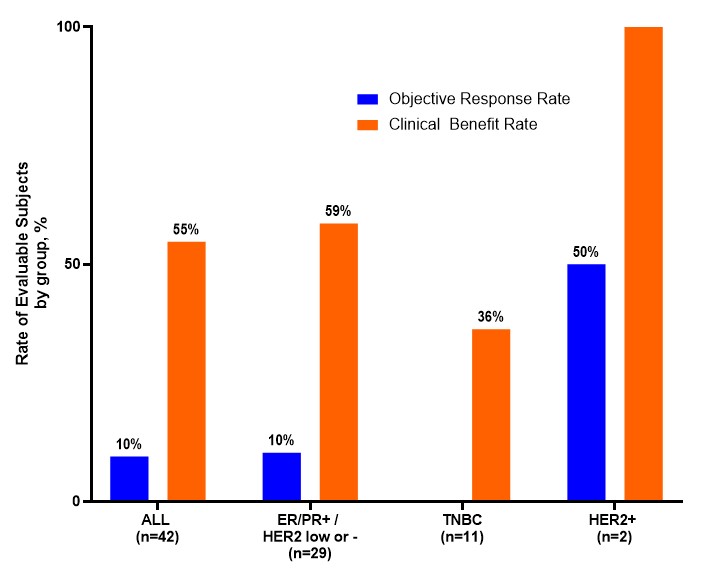
Clinical benefit was seen in 55% of evaluable patients across all subtypes of breast cancer as shown in Figure 2 below.
Figure 2: Objective Response Rate (ORR) and Clinical Benefit Rate (CBR) in the Bria-IMT™ Phase 1/2 Study
The progression free survival rate and the clinical benefit rate as well as the objective response rate were markedly higher than those of similar patients treated with the treatment of their physician’s choice in other studies. Notably, “Treatment of Physician’s Choice” (TPC) will be the comparator in the Phase 3 study of Bria-IMT™. This is noted in Table 2 below.
| Table 2. Comparative PFS, ORR and CBR in Similar Patients | ||||
| Study | Prior Lines of Therapy (median, range) |
PFS (months) |
ORR (%) |
CBR (%) |
| BriaCell’s Phase 2 study patients who received pivotal Phase 3 study formulation | 6 (2-13) | 3.9 | 9.5* | 55* |
| BriaCell’s ADC Resistant Phase 2 patients who received pivotal Phase 3 study formulation | 6 (3-13) | 4.1 | 12** | 53** |
| Bardia, A. et. al. 1 | 4 (2-14) | 1.7 | 4 | 8 |
| Tripathy D. et. al. 2 | ≥4 in 91% | 1.9 | 3 | 10 |
| O’Shaughnessy J. et. al. non-TNBC 3 | 5 (2-14) | 2.3 | 4 | 7 |
| O’Shaughnessy J. et. al. TNBC 3 | 4 (2-10) | 1.6 | 5 | 10 |
*Data is for evaluable patients, n=42 with 12 not evaluable.
** Data is for evaluable patients, n = 17 with 6 not evaluable.
References: Data is shown for the intent to treat population for the control group treated with treatment of physician’s choice, which is the comparator in the BriaCell Phase 3 study
1. Bardia A, et al. J Clin Oncol. 2024 May 20;42(15):1738-1744.
2. Tripathy D, et al. JAMA Oncol. 2022 Nov 1;8(11):1700-1701. jamaoncol.2022.4346. PMID: 36136348. This paper describes patients with brain metastases.
3. O’Shaughnessy J, et al. Breast Cancer Res Treat. 2022 Sep;195(2):127-139.
For additional detailed information of the clinical data on the oral presentation, please visit BriaCell Doubles Progression-Free-Survival (PFS) and Reports Clinical Benefit Data at ASCO 2024 .
Poster Presentation Summary
The first poster described BriaCell’s ongoing pivotal Phase 3 registrational study in advanced metastatic breast cancer. BriaCell is excited to collaborate on this important program with authors and BriaCell medical advisory board members Sara A. Hurvitz, MD, Professor of Medicine, Fred Hutchinson Cancer Center, Adam M. Brufsky, MD, PhD, Professor of Medicine, University of Pittsburgh School of Medicine, and Massimo Cristofanilli, MD, Professor of Medicine, Weill Cornell Medical College, Cornell University. The second poster described clinical data of Bria-IMT™ in metastatic breast cancer patients who failed antibody drug conjugates (ADCs) and is spearheaded by Chaitali Nangia, MD, Partner, Hoag Medical Group, and Carmen Calfa, MD, Professor of Medicine, University of Miami.
Abstract Number for Publication: TPS1137
Title: Study of the Bria-IMT™ regimen and CPI vs physicians’ choice in advanced metastatic breast cancer (BRIA-ABC).
Based on Phase 2 clinical data showing numerous survival and clinical benefit outcomes in advanced breast cancer patients treated with the Bria-IMT™ regimen, the pivotal Phase 3 study has been designed as a multicenter randomized, open label comparison of the Bria-IMT™ regimen plus CPI in one arm versus Treatment of Physicians’ Choice (TPC) in metastatic breast cancer patients with no approved alternative therapies available. Patients’ eligibility includes treatment with 2 or more prior regimens. There will be another arm of the Bria-IMT™ regimen alone (monotherapy). For additional information on the pivotal Phase 3 study, please visit ClinicalTrials.gov as NCT06072612 .
Abstract Number for Publication: 1087
Title: SV-BR-1-GM after progression on ADC in patients with metastatic breast cancer.
Remarkable progression-free survival and clinical benefit of Bria-IMT™ in ADC resistant advanced metastatic breast cancer
Phase 2 clinical data of the Bria-IMT™ regimen in 23 advanced metastatic breast cancer patients who failed multiple prior treatments including ADCs and CPIs (median of 6 prior treatments) are presented.
Clinical efficacy
- In evaluable patients, the ORR was 12% and CBR was 53% which is remarkable versus similar data suggesting clinical benefit.
- Median PFS of 4.1 months with the Phase 3 formulation was ~twice that seen of patients in similar studies – 1.7 1 and 2.2 3 months – who received TPC. The PFS results suggest superior clinical efficacy given the larger number of prior treatments (median of 6) in Bria-IMT™ patients vs those of the other studies (median of 4).
- Subset specific clinical benefits : Study data to date suggests clinical benefit for multiple breast cancer subtypes including HR+/HER2- (the most common breast cancer subtype, testing positive for estrogen and/or progesterone receptors and negative for human epidermal growth factor receptor 2 or HER2) with a CBR following treatment, of 63% (5 of 8 patients); HER2+ subtype (a positive test for HER2) with a 100% CBR (2 of 2 patients) and HR-/HER2 low subtype (a negative test for estrogen and/or progesterone receptor and a negative test for HER2) showing a CBR of 66% (2 of 3 patients). See Table 3.
| Table 3: Treatment Efficacy by Metastatic Breast Cancer Subtype in ADC-resistant patients | ||||
| Histology | All Patients (N) | Evaluable (N) Patients | Best ORR | Best CBR |
| All ADC Resistant | 23 | 17 | 12% (2 / 17) | 53% (9 / 17) |
| ER/PR + / HER2 low or – | 8 | 8 | 13% (1 / 8) | 63% (5 / 8) |
| HER2+ | 3 | 2 | 50% (1 / 2) | 100% (2 / 2) |
| TNBC | 12 | 7 | 0 | 29% (2 / 7) |
- Bria-IMT™ showed potential survival advantage over penultimate treatment in 48% of patients, likely by reversing immune exhaustion in patients irrespective of specific prior ADC.
Safety profile
Absence of both interstitial lung disease (ILD), a common serious adverse event with ADCs, and Bria-IMT™-related treatment discontinuations underscore Bria-IMT™’s excellent tolerability and favorable safety profile.
In summary, the data to date shows that Bria-IMT™ offers extended progression-free survival and clinical benefit in heavily pre-treated, ADC resistant breast cancer patients versus those in other similar studies. BriaCell is closely monitoring ADC resistant patients in its ongoing pivotal Phase 3 study of Bria-IMT™ and CPI in advanced metastatic breast cancer.
Title: Differential efficacy of SV-BR-1-GM in inducing intracranial metastasis regression.
Superior clinical benefit of Bria-IMT™ regimen – alone or combined with an immune check point inhibitor (CPI) in advanced breast cancer patients with CNS metastatic disease
Central nervous system (CNS) metastases, including brain metastases and other intracranial metastases, is a dire clinical situation with very poor survival. Very few therapies have shown any effect on CNS or intracranial metastases in breast cancer and it is a serious unmet medical need.
Clinical efficacy:
- 83% (5/6) intracranial objective response rate (iORR) was reported in evaluable patients with central nervous system (CNS) metastases treated with the Bria-IMT™ regimen, either alone or in combination with an immune checkpoint inhibitor (i.e. PD-1 inhibitor pembrolizumab or retifanlimab). These patients failed multiple prior treatments including 2 antibody-drug conjugates in one case. This is illustrated in Figure 3.
Figure 3. Intracranial Tumor Responses in Patients with Intracranial Metastases Treated with Bria-IMT™
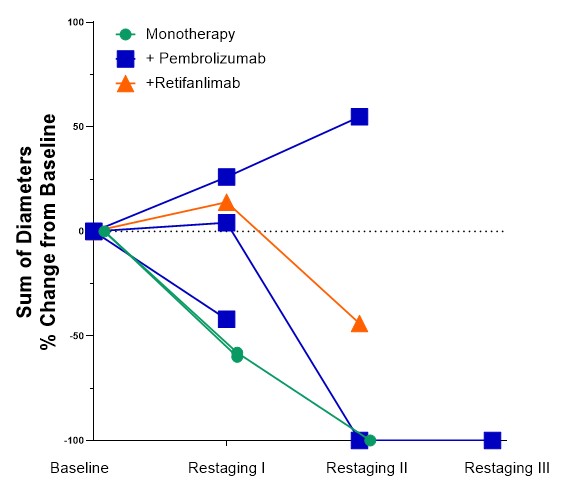
- Tumor reductions (≥30% reduction in the sum of diameters) were observed in heavily pretreated patients highlighting potential clinical benefit of Bria-IMT™ in managing CNS metastases
- This is a pre-planned subgroup analysis in the pivotal Phase 3 study of Bria-IMT™ providing another opportunity for approval
Safety profile:
No treatment related discontinuation was reported.
In summary, Bria-IMT™’s tumor reductions observed in patients with intracranial disease underlines its potential clinical effectiveness in managing CNS metastatic disease in advanced breast cancer. BriaCell will continue to monitor the data in this subgroup of patients in its ongoing pivotal Phase 3 study in advanced metastatic breast cancer. Treatment of patients with CNS metastatic disease represents a potential additional indication for market approval of Bria-IMT™.
Copies of the poster presentations and abstracts are posted on https://briacell.com/scientific-publications/ .
References
- Bardia A, et al. Final Results From the Randomized Phase III ASCENT Clinical Trial in Metastatic Triple-Negative Breast Cancer and Association of Outcomes by Human Epidermal Growth Factor Receptor 2 and Trophoblast Cell Surface Antigen 2 Expression. J Clin Oncol. 2024 May 20;42(15):1738-1744. doi: 10.1200/JCO.23.01409. Epub 2024 Feb 29. PMID: 38422473.
- Tripathy D, et al. Treatment with etirinotecan pegol for patients with metastatic breast cancer and brain metastases: final results from the Phase 3 ATTAIN randomized clinical trial. JAMA Oncol. 2022;8(7):1047-1052. doi:10.1001/jamaoncol.2022.0514.
- O’Shaughnessy J et al. Analysis of patients without and with an initial triple-negative breast cancer diagnosis in the Phase 3 randomized ASCENT study of sacituzumab govitecan in metastatic triple-negative breast cancer. Breast Cancer Res Treat. 2022 Sep;195(2):127-139. doi: 10.1007/s10549-022-06602-7. Epub 2022 May 11. PMID: 35545724; PMCID: PMC9374646.
About BriaCell Therapeutics Corp.
BriaCell is a clinical-stage biotechnology company that develops novel immunotherapies to transform cancer care. More information is available at https://briacell.com/ .
Safe Harbor
This press release contains “forward-looking statements” that are subject to substantial risks and uncertainties. All statements, other than statements of historical fact, contained in this press release are forward-looking statements. Forward-looking statements contained in this press release may be identified by the use of words such as “anticipate,” “believe,” “contemplate,” “could,” “estimate,” “expect,” “intend,” “seek,” “may,” “might,” “plan,” “potential,” “predict,” “project,” “target,” “aim,” “should,” “will,” “would,” or the negative of these words or other similar expressions, although not all forward-looking statements contain these words. Forward-looking statements, including those about the presentation at the 2024 ASCO of two poster sessions, one abstract, and the delivery of an oral presentation by Dr. Saranya Chumsri, and the contents of all such materials and presentations; BriaCell’s novel immunotherapy offering a well-tolerated treatment option for patients beyond the currently approved drugs; Bria-IMT™ having the potential to become a breakthrough novel treatment option for patients in advanced metastatic breast cancer; “Treatment of Physician’s Choice” (TPC) being the comparator in the Phase 3 study of Bria-IMT™; monotherapy becoming another arm of the Bria-IMT™ regimen; the potential clinical benefit of Bria-IMT™ in managing CNS metastases disease in advanced breast cancer; BriaCell continuing to monitor the data in the intracranial disease subgroup of patients in its ongoing pivotal Phase 3 study in advanced metastatic breast cancer; and the treatment of patients with CNS metastatic disease representing a potential additional indication for market approval of Bria-IMT™, are based on BriaCell’s current expectations and are subject to inherent uncertainties, risks, and assumptions that are difficult to predict. Further, certain forward-looking statements are based on assumptions as to future events that may not prove to be accurate. These and other risks and uncertainties are described more fully under the heading “Risks and Uncertainties” in the Company’s most recent Management’s Discussion and Analysis, under the heading “Risk Factors” in the Company’s most recent Annual Information Form, and under “Risks and Uncertainties” in the Company’s other filings with the Canadian securities regulatory authorities and the U.S. Securities and Exchange Commission, all of which are available under the Company’s profiles on SEDAR+ at www.sedarplus.ca and on EDGAR at www.sec.gov . Forward-looking statements contained in this announcement are made as of this date, and BriaCell Therapeutics Corp. undertakes no duty to update such information except as required under applicable law.
Neither the Toronto Stock Exchange nor its Regulation Services Provider (as that term is defined in the policies of the Toronto Stock Exchange) accepts responsibility for the adequacy or accuracy of this release.
Contact Information
Company Contact:
William V. Williams, MD
President & CEO
1-888-485-6340
info@briacell.com
Media Relations:
Jules Abraham
CORE IR
julesa@coreir.com
Investor Relations Contact:
CORE IR
investors@briacell.com
Photos accompanying this announcement are available at
https://www.globenewswire.com/NewsRoom/AttachmentNg/6fff10ca-4660-4c6f-bb46-719f0f21887d
https://www.globenewswire.com/NewsRoom/AttachmentNg/2b7cbddb-da76-486d-b6c3-22894a42933a
https://www.globenewswire.com/NewsRoom/AttachmentNg/66f03119-a4b3-4d2d-a998-ab355aefdeac
